Dental studnet University of New England College of Dental Medicine Portland, Maine, United States
Disclosure(s):
Sean W. Noll: No financial relationships to disclose
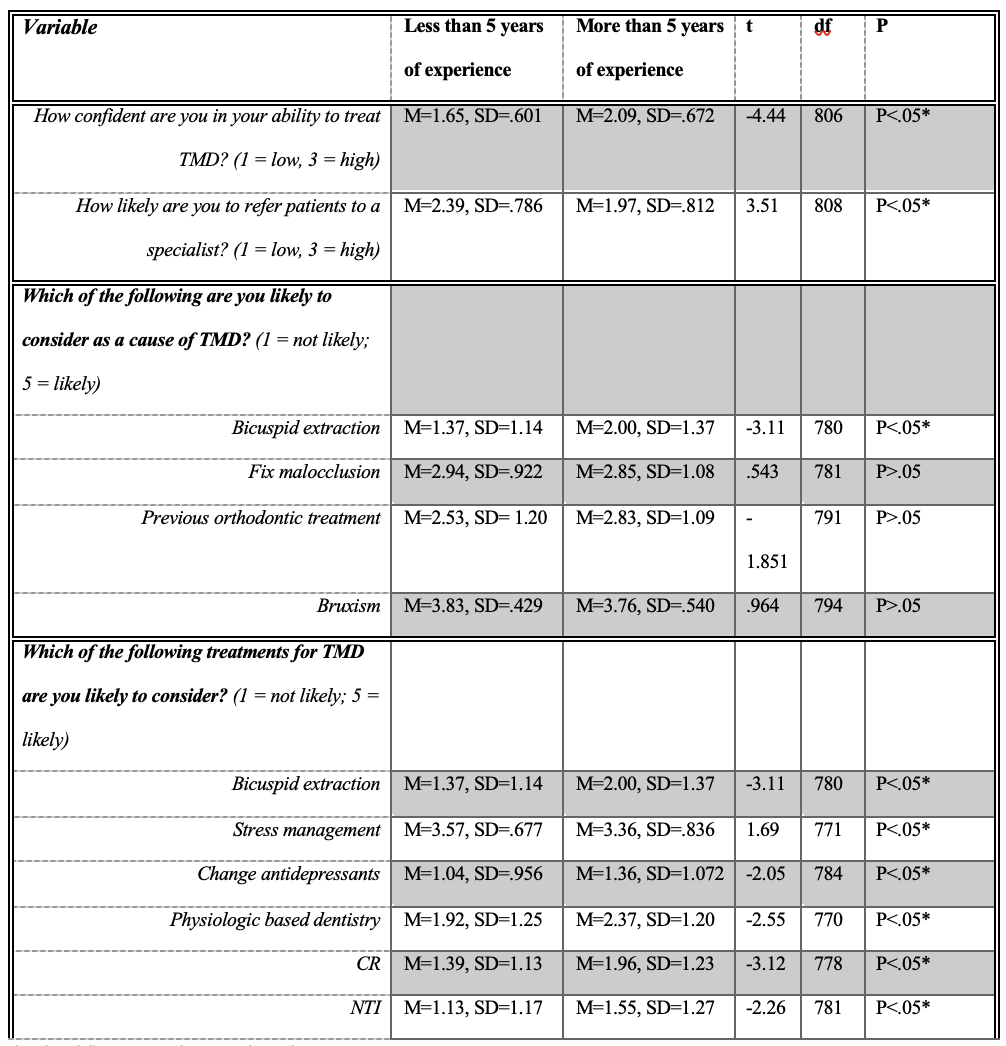
Abstract: Temporomandibular joint disorder (TMD) refers to a broad, multifaceted group of over 30 different diagnoses that involves pain and disfunction of the temporomandibular joint (TMJ). Treatment options are highly debated due to limited and mixed empirical evidence. This study surveyed all licensed Ohio dentists (n = 7,573) via email to evaluate assumptions about causes and treatment preferences for TMD. Responses collected totaled 826, with almost half of the respondents (n = 414) having attended a residency program after dental school. Dentists in practice longer than 5 years felt more confident in treating TMD and were more likely to treat TMD with physiologic based dentistry, NTI, and CR dentistry — even though the literature indicates that these methods are no longer preferred. They also were more likely to view bicuspid extractions as a cause, compared to dentists practicing less than 5 years. Dentists in practice less than 5 years were more likely to refer TMD patients to another practitioner or specialist. Additionally, they were more likely to treat TMD with stress management and corticosteroid or botulinum toxin type A injections. There was no significant difference in their identification of fixing malocclusions as a treatment. They also rated previous orthodontics and bruxism similarly as possible causes. See Table 1 for their response means, standard deviations, and the independent t-test results. The survey showed that many dentists were still using treatment plans that are non-evidence based or described in the literature as obsolete. Oral appliances (OA) are currently an accepted standard of care for TMD, and practitioners are attempting to treat any of the 30+ TMD conditions with such devices. OAs have been shown to cause significant improvement of symptoms in a majority of studies. However, there are many instances where an integration of other forms of treatments are needed. Overall, current evidence-based treatment plans recommended by orofacial pain specialists align with the biopsychosocial model and include psychological factors that incorporate the etiology of TMD.ReferencesCommittee on Temporomandibular Disorders (TMDs): From Research Discoveries to Clinical Treatment, Board on Health Sciences Policy, Board on Health Care Services, Health and Medicine Division, & National Academies of Sciences, Engineering, and Medicine. (2020). Temporomandibular Disorders: Priorities for Research and Care (E. C. Bond, S. Mackey, R.Michelotti, A., Rongo, R., D'Antò, V., & Bucci, R. (2020). Occlusion, orthodontics, and temporomandibular disorders: Cutting edge of the current evidence. Journal of the World federation of orthodontists, 9(3S), S15–S18. https://doi.org/10.1016/j.ejwf.2020.08.003Menchel, H. F., Greene, C. S., & Huff, K. D. (2021). Intraoral appliances for temporomandibular disorders: What we know and what we need to know. Frontiers of Oral and Maxillofacial Medicine, 3, 6–6. https://doi.org/10.21037/fomm-20-49
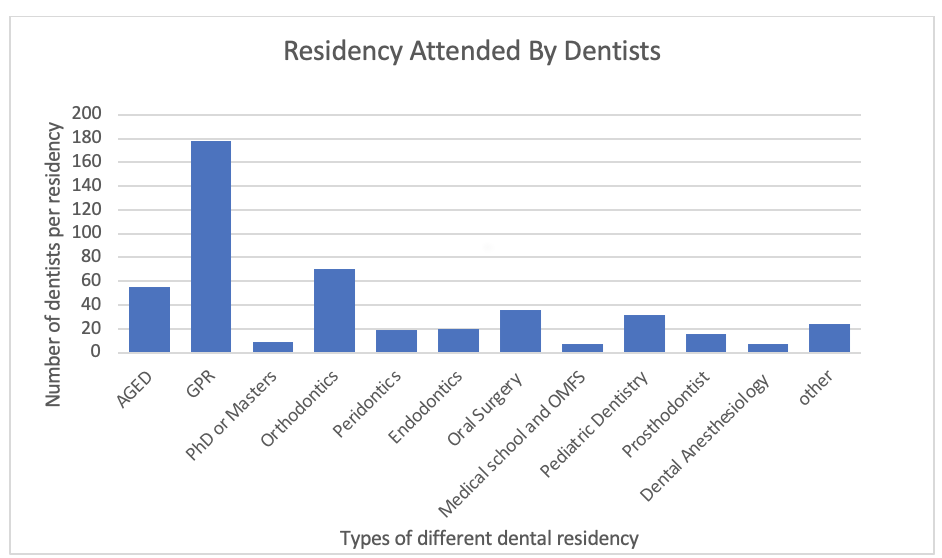
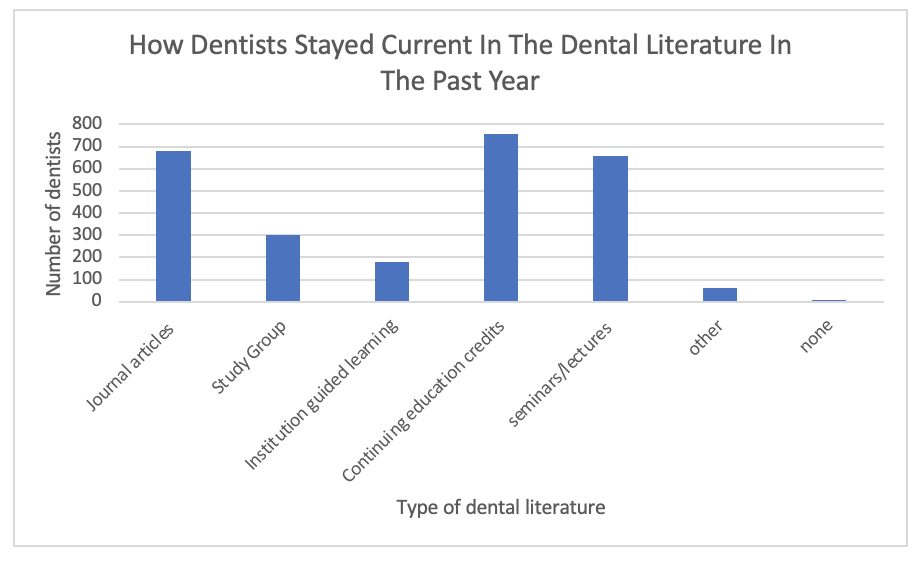
Figure 1: Breakdown of dentists that attended a residency. 414 dentists responded yes and 409 responded no to attending a residency Figure 2. Resources dentists used to stay current in the dental literature. Table 1: Inferential statistics on treatments and causes between dentists working more than 5 years and less than 5 years.

 photo")